ADCs: Pros and Cons
This is the third article in a series of five blog posts that are putting ADCs in the spotlight. This article will describe the pros and cons of the ADC drug class. Please read the introductory post ADCs: What are they and why do they matter? before this post, if you are unfamiliar with ADCs.
Look out for; ADCs: Origins and Obstacles, and ADCs: Pipeline and Progress, coming soon.
Pros
ADCs combine the targeting ability of mAbs with the cytotoxic power of small molecule drugs. ADCs are however, more than just the sum of their parts.
The high specificity of an ADC to its target receptor and combined with the controllable warhead activation and release mechanisms, result in ADCs having significantly less off target action compared to a therapeutically comparable small molecule cytotoxic. Consequently more patients are likely to tolerate ADC regimes. The higher specificity and controllable release mechanisms, ensure more drug successfully reaches the targeted cells, meaning lower concentrations are required to elicit an equivalent therapeutic response compared to antibody, small molecule co-therapy. These two principles give ADCs a wider therapeutic window, potentially making it useful in patients who can no longer tolerate combination therapy, or useful in patients who are no longer responding to combination therapy.

Resistance to ADCs takes longer to develop than resistance to their constituent mAb. Therry et al [1] reviewed methods of resistance to trastuzumab and lapitinib. While alteration or truncation of the HER2 extracellular domain could result in resistance to trastuzumab emtansine and trastuzumab, most methods of resistance to trastuzumab are due to changes in signalling downstream of HER2. Changes to signalling pathways would not prevent the payloads accumulating and destroying the cells. This means it should take longer for a relevant method of resistance to occur. The increased duration before resistance develops and wider therapeutic window, allow ADCs to fight cancers harder and longer than ever before, which accounts for the impressive therapeutic power of ADCs
Cons
ADCs are still subject to resistance, thus have a limited duration of effectiveness. ADCs must target extracellular receptors, that are endocytosed, to transport the payloads inside the cells. These extracellular receptors may not be exclusively found on the target cell population, while systemic activity may be low there could be unwanted toxicity at another population of cells that also has the targeted receptors present. Also multi-drug resistance pumps (MDRPs) actively remove released warheads. Mutations increasing MDRP expression, activity or reducing selectivity of MDRPs can increase the rate of developing resistance to ADCs.

ADCs are heterogeneous, with variable drug to antibody ratio (DAR) and distribution of payloads (DOP). This is because linkers bind to lysines or cysteines in the mAb which are present in greater abundance than payloads will bind. This increases potential variability in stability, pharmacokinetics and activity. ADCs with a DAR of 0 or 1 will reduce average potency, as they could bind in place of an ADC with a higher DAR. Furthermore certain DOPs will also have lower activity than others, potentially interfering with Fab or Fc region binding. The DAR and DOP variability increases the dose required for desired therapeutic effect, increases off target effects and increases the cost of therapy.
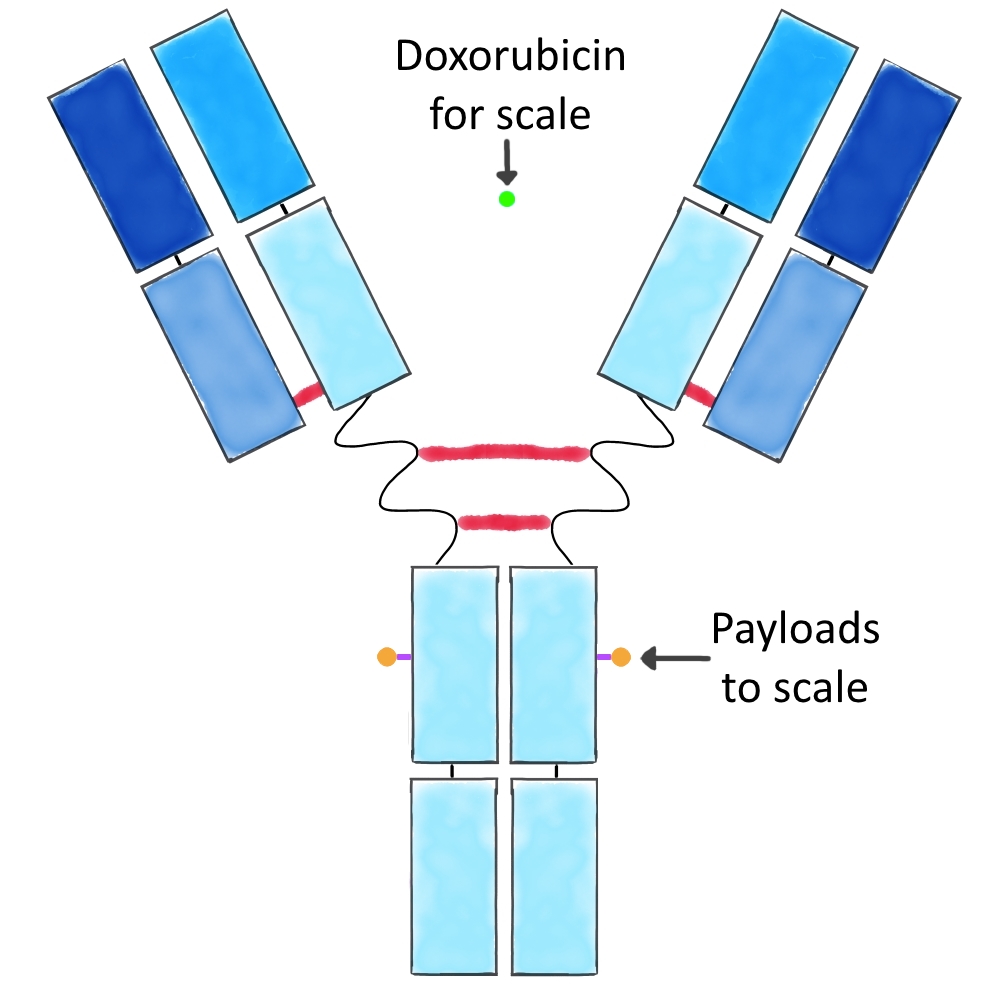
ADCs are also huge compounds, over 150kD, while conventional cytotoxics such as doxorubicin are less than 0.6kD. Their size makes it harder for ADCs to penetrate solid tumours, and less available at their intended site of therapeutic action.
Summary
ADCs have clear advantages over current mono and combination therapies, but also have clear disadvantages. The advantages demonstrably outweigh the disadvantages for trastuzumab emtansine in the treatment of HER2+ breast cancer. Expect more ADCs to be licensed as our understanding of this technology improves and allows us to diminish the disadvantages for future ADCs.
References
- Thery JC, Spano JP, Azria D, Raymond E, Penault Llorca F. Resistance to human epidermal growth factor receptor type 2-targeted therapies. Eur J Cancer. 2014 Mar;50(5):892-901.